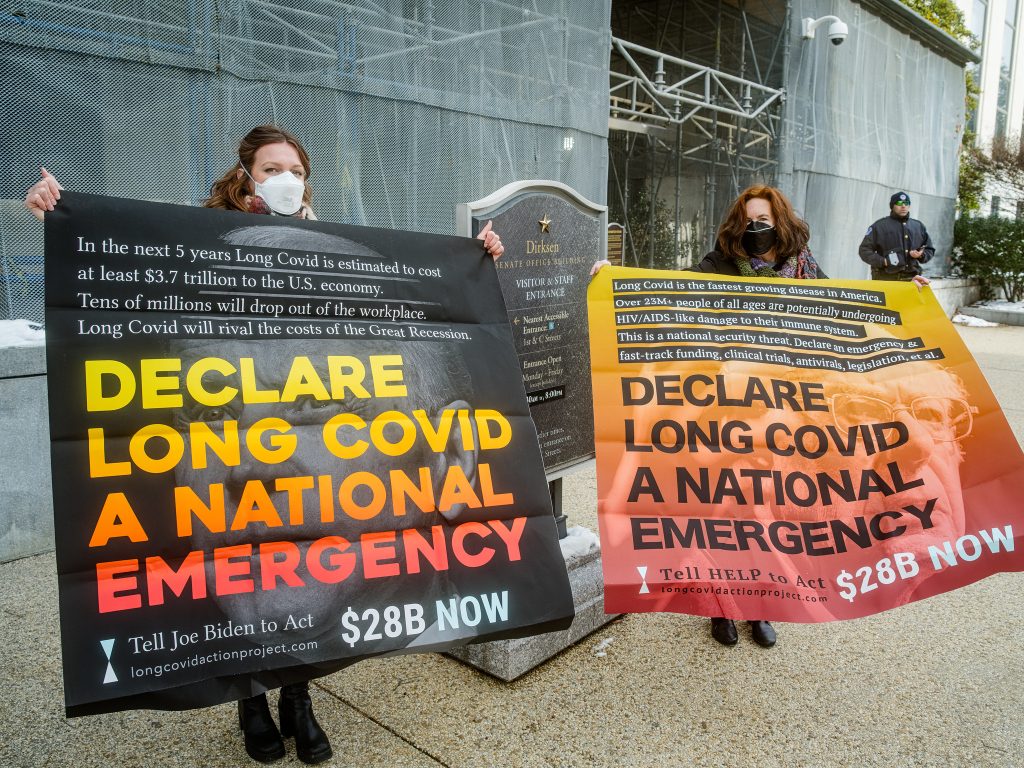
Long COVID patients suffer from the same societal attitudes that affect many people with invisible and fluctuating disabilities
~ Fingers Malone ~
The government’s “let it rip” attitude to COVID-19 led to the preventable death of large numbers of people, most infamously vulnerable elderly people in care homes. Lack of protections for vulnerable people, failure to provide adequate PPE, and forcing people to work in dangerous conditions exposed many people unnecessarily to the virus. It has also led to large numbers of people now suffering long COVID.
Long COVID can cause a wide range of symptoms but the most common are fatigue, brain fog, muscle aches and breathlessness. Fatigue is not just feeling tired, but is a very debilitating condition that can leave people unable to walk or take a shower without help. Women are more likely to develop it than men, and it’s most common in the 45-54 age group.
The newspapers, when they cover long COVID at all, are now reporting that patients have mostly gotten better (not the case) and that the current strains are not as dangerous. Having up-to-date boosters does provide some protection (so it is scandalous that the government is not providing free boosters to the general population) and the especially virulent early strains are more likely to lead to long covid than the later variants. However nobody is immune and every COVID infection still has a risk. Immunocompromised people are especially at risk of their condition getting worse with reinfection, which makes the current “COVID is over” assumptions very difficult to navigate for people.
Long COVID sufferers, and other people who are especially vulnerable to COVID infection, are currently having to deal with a situation where buildings do not have air purifiers, people do not wear masks anywhere even in hospitals, employers are telling people to come to work with COVID, basically vulnerable people are written off and told to deal with the risk by themselves.
Some people wearing masks are abused on buses. Others have said they are marked down as difficult patients for asking staff to wear masks on hospital visits. Doctors are too inclined to write off long COVID as ”just a mental health condition”. The push for attendance in schools, including telling children to come in when they are sick, puts both children and staff who are vulnerable at risk of infection, and puts pressure on pupils with any chronic illness to attend to the detriment of their health.
Doctors like patients to come in with a condition that has a straightforward test and then a recognised treatment plan and there is often mistreatment and neglect of patients with conditions that don’t fit this model.
Long COVID patients suffer from a lot of the same societal attitudes that affect many people with invisible and fluctuating disabilities. Many people perceive “genuine” disabilities to exist only when a person cannot do anything at all and when their condition is always the same. A classic example is that a wheelchair user should not be able to move their legs — there was a lot of fuss when Doctor Who had a character in a wheelchair who crossed hers. This actor, in real life, does use a wheelchair, and she can cross her legs. Many people who use wheelchairs can walk short distances, and people are afraid to get out of their wheelchairs in public due to hostile reactions. The only criteria for whether somebody has the “right” to use a wheelchair is if that person benefits from using a wheelchair, and bystanders can mind their own business.
Long COVID is a post-viral condition and these are not new or unknown, after the SARS epidemic large numbers of patients were ill long term with them. The government was warned about this by scientists when COVID started, but appear to have ignored it. A lot of patients reporting feeling ill after the acute infection passed were told by GPs to exercise, which is now understood to be harmful.
People underestimate the prevalence of long COVID for various reasons. Many who have long COVID don’t know it, as they don’t connect a COVID infection months ago with what appears to be a separate health problem that has turned up. There isn’t a straightforward long COVID test, or at least not one that GPs are habitually using. People who are not well enough to work and be part of social activities drop out of sight of everyone except people who make the effort to stay in contact with them.
The treatment of patients with ME or chronic fatigue is very relevant to long COVID patients. ME was identified in the 1950s at a London hospital and was considered from the start to be a real condition with a physical cause. It was studied and investigated as a post-viral condition. The widely held view of ME as fake, basically hysteria, comes from the views of a small number of scientists who have been given a lot of legitimacy by the government, who preferred to be dismissive of other scientists because it meant they could just ignore and disregard ME patients. The shocking mistreatment of ME patients is a very serious injustice and long COVID patients need to be in solidarity with them struggling for research and compassionate medical treatment.
The government’s increasingly shrill announcements that too many people are “economically inactive” and about returning the long term sick to the workplace are causing anxiety and fear amongst sick and disabled people of all conditions. People being pushed into work that they can’t do can cause serious damage to their health. Reports on long COVID minimising the severity of the condition is in this context very worrying. Many long COVID patients have lost their jobs due to their employers refusal to make accommodations, and many others are too sick to work even with accommodations.
The government likes to announce yet more crackdowns on claimants, crackdowns that increase hostility, including violent attacks on disabled people, but don’t tackle workplace discrimination, inaccessible transport and lack of accommodations.
Clean air inside buildings, especially hospitals and schools, would do a lot to prevent COVID spread. Masking in key places such as hospitals would help protect the most vulnerable. This society is not a caring and supportive place for people with a chronic health condition. Our movement should be, but in practice isn’t always much better. People who have become disabled by a virus need support with rest and recovery, not judgement about whether they are really trying hard enough.
Covid safety is difficult to think about for people who feel burned out after years of the pandemic, but immunocompromised people can’t be treated as disposable. Thinking about and including people with long COVID will involve measures that are helpful for lots of other people as well. Air purifiers help people with allergies, bringing a chair to pickets helps people with bad knees or who are pregnant.
Ill health isn’t a moral failure or people being annoying, the vulnerability of the body is a part of being human.
This article first appeared in the Winter 2024/25 issue of Freedom Anarchist Journal
To read more about the anarchist and mutual aid approaches during the pandemic, check out Fight For a New Normal?